
It has been six months since ACC/AHA changed the hypertension(HTN) guidelines, effectively reclassifying 31 million more US adults from ‘high or elevated blood pressure’ to HTN.
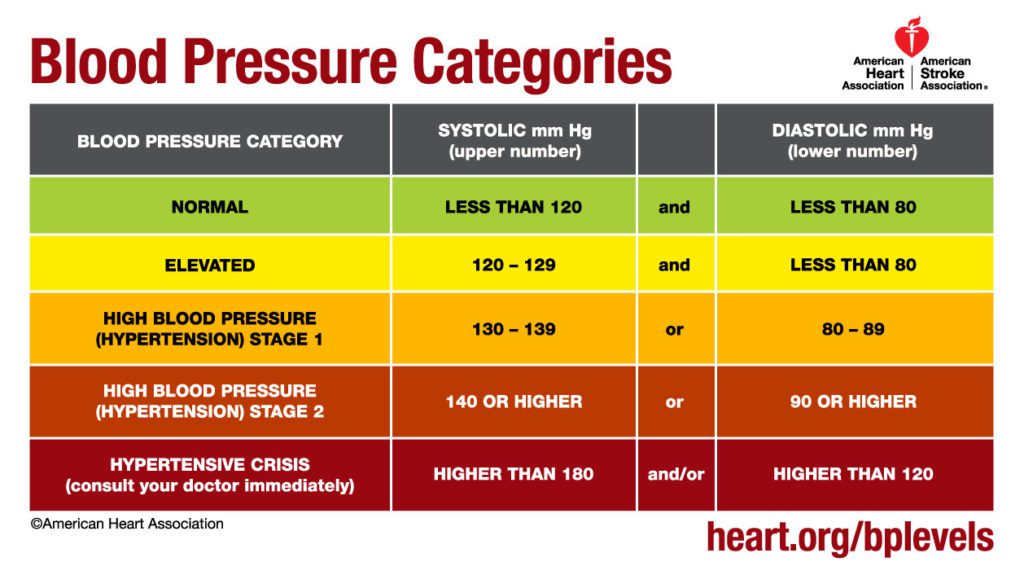
The new hypertension guidelines define HTN Stage 1 as systolic from 130-139 or HG diastolic from 80-89 mm. Previously, HTN was categorized as 140/90 or higher.
New Hypertension Guidelines Expected to Effect Patients, Doctors, and Hypertension Related Prescriptions
The American College of Cardiology reports that Paul Muntner, PHD et al.’s corresponding analysis suggests “the 2017 ACC/AHA hypertension guideline has the potential to increase hypertension awareness, encourage lifestyle modification and focus antihypertensive medication initiation and intensification on US adults with high CVD risk.”
The New Hypertension Guidelines
With 4.2 million more patients being recommended for immediate drug treatment for HTN according to the guideline, there are others who view it differently.
Dr. Katy Bell of the University of Sydney, lead author of a study on the incremental benefits and harms of the guideline published by Jama Internal Medicine, raises concerns about the hypertension guideline change. In her and her co-author’s list of concerns, shared on EurekAlert! with Dr. Bell herself listed as the media contact, it points to the risk of ADEs and states:
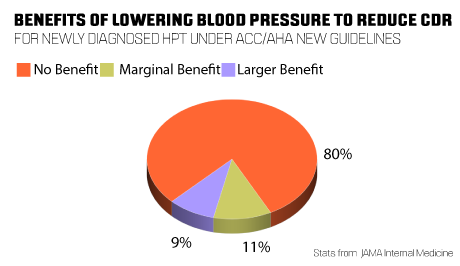
“The report says 80 per cent of people with newly diagnosed hypertension under the ACC/AHA guideline would get no expected benefit in terms of cardiovascular disease risk reduction by lowering their blood pressure. Eleven per cent would get a marginal benefit and nine per cent would get a larger benefit.”
While there is expected to be only a “small increase in the percentage of U.S. adults recommended antihypertensive medication,” the population already taking antihypertensive medication will now be recommended more intensive BP lowering medication under the new guideline. This group may be more substantially impacted by the guideline change.
PEPID’s in-house medical editors had this to say:
“Lowering the threshold (i.e. increasing sensitivity) may change protocols to some/many hospital plans for patients. With a wider reach of potential patients, HTN drug prescribing may increase – as we’ve seen with lowering the threshold for Diabetes (A1c).
Granted, guidelines do not always dictate physician discretion. However, if the HTN threshold lowering does prove profitable and not harmful to patients, we may see more changes to protocols for the treatment of HTN, in effect, we may also see an increase in prescribing HTN drugs. Time will tell. “
– Nick (Nghia) Ho, MD, Medical and Pharma Informatics Lead Editor
“I think it is important to highlight the fact that guidelines are simply that, guidelines. They serve to provide direction for the practitioner as it relates to patient diagnosis and management, but guidelines are not meant to be applied to every single patient. The need for individualized management is typically emphasized when guidelines are announced. Whether or not such patients will be officially diagnosed as having HTN will be at the discretion of the practitioner. Further, whether or not these patients will be treated with newly prescribed medications (as opposed to lifestyle modifications alone) is ultimately the decision between the patient and physician – given the patient’s medical history.
As far as diagnostic criteria go, they do change from time to time so it will be interesting to see how these new BP/HTN definitions hold up against the test of time (and against the test of practitioner feedback and patient outcome).”
–James Hernandez, DO, Medical Informatics Editor
As both Dr. Ho and Dr. Hernandez point out, ultimately the goal and responsibility of clinicians remains the same with any modification of guidelines: improve the health of the patient.